Clinical Research
Thank you for visiting the website of P&S Mechanics Co., Ltd.
Thank you for visiting the website of P&S Mechanics Co., Ltd.
Although ankle robotic control has emerged as a critical component of robot-interactive gait training (RIGT), no study has investigated the neurophysiological and biomechanical effects on ankle muscle activity and joint angle kinematics in healthy adults and participants with brain damage, including stroke and cerebral palsy (CP). This study compared the effects of RIGT, with and without ankle robotic control(actuator), on ankle muscle activity and joint angle kinematics in healthy adults and participants with brain damage. Descriptive statistical analysis demonstrated that RIGT with ankle control actuator showed superior effects on EMG (30%) and kinematics angles (25%) than RIGT without ankle control actuator.
Our results provided novel, promising clinical evidence that RIGT with ankle control actuator can more effectively improve the neurophysiological EMG data and ankle dorsiflexion and plantarflexion movements than RIGT without ankle control actuator in participants with stroke and CP.
Insufficient ankle–knee–hip joint coordination is a common neuromechanical impairment in millions of patients with brain damage because it can result in a serious fall injury. As many as 77%–80% of the participants with brain injury experience fatal falls, which can lead to death. In particular, limitedselective ankle movement during locomotion has been accounted for as the main reason for the loss of balance during independent activities of daily living and the associated serious falls. Neuromechanically, the ankle musculature plays a cardinal role in the forward momentinduced propulsion during mid-to-late stance, toe clearance in the swing phase, and shock absorption at initial contact (IC) of the gait cycle. Pathomechanically, some (or all) of these neuromechanical aspects of gait are impaired following a brain damage. The paretic or weak tibialis anterior (TA) is unable to activate effectively to clear the toe or the foot during IC and swing phases.
Currently commercialized exoskeletal robotics including Lokomat (Hocoma, Volketsiwl, Switzerland) and ALTACRO (Vrije Unviersiteit, Brussel, Belgium) present one major limitation that patient’s legs move passively along a predefined trajectory without actively influence their movements. To mitigate this problem, we have developed an innovative ankle–knee–hip joint coordination robot-interactive gait training system (RIGT; also known as Walkbot G, P&S Mechanics, Seoul, Republic of Korea), which is capable of providing an independent ankle control actuator in addition to hip and knee actuators for foot clearance; this device assists the hip, knee, and ankle joints movement in the sagittal plane when combined with a motorized treadmill and body weight support.
Despite the clinical importance of the role of the ankle joint control during the RIGT intervention paradigm, no previous study has compared the potential clinical benefits and the underlying neuromechanical relationship between the RIGT with and without ankle control actuator. Therefore, we proposed to compare the effect of RIGT with and without ankle control actuator on TA and gastrocnemius (GCM) muscle activity and joint kinematics in participants with stroke or cerebral palsy (CP).
The Walkbot is an RIGT device, which is designed to perform under different control modes, including passive, active-assistive modes that modify the control parameters based on the ongoing participant’s performance and real-time audiovisual biofeedback for torque and stiffness, in addition to kinematics support for the hip, knee, and ankle joints during gait training. The target locomotor trajectory is predefined in the passive mode, and participants depend on the robot. The device consists of a suspension harness for a bodyweight system, a motorized treadmill, and an actuatorcontrolled exoskeleton. The motorized treadmill speed and torque (assistance and resistance) can be adjusted to provide the user with safe and challenging locomotor retraining modes as the training progresses.
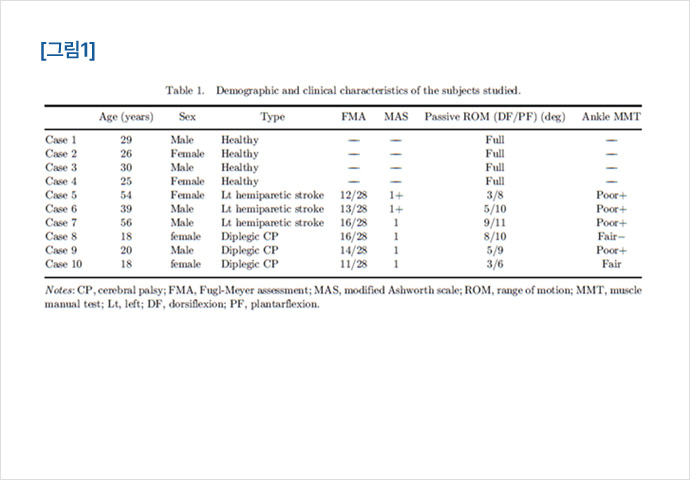
The sample of 10 participants (four healthy adults, three patients with CP, and three with left hemiparetic stroke patients) was recruited for this study.
All participants underwent clinical tests, surface electromyography (EMG), and kinematics measurements for both ankle joint motion and muscle activity. However, the data were compared for the dominant side in the healthy subjects and the affected side in articipants with hemiparetic stroke and CP, respectively. Primary clinical tests included Fugl-Meyer assessment of lower extremity (FMA-LE), modified Ashworth scale (MAS), range of motion (ROM), and manual muscle test (MMT).
All participants received a single 30-min RIGT session, which was sufficient for familiarization with and testing the procedure. RIGT was provided with the Walkbot RIGT system, which was equipped with independent and coordinated ankle, knee, and hip joint actuator control during gait training. Walkbot RIGT can provide systemic assistance or resistance interactively in response to the patient’s muscle strength, movement and fatigue conditions during gait training. Furthermore, independent ankle control actuator sensors can selectively isolate the ankle dorsiflexion and plantarflexion joint movement in difference to other RAGT systems, such as the Lokomat. Approximately 40%–60% of the body weight was sustained following the participant’s clinical conditions (e.g., pain, muscle weakness, spasticity, and fatigue) and progressively decreased by 5%–10% per minute. Walking velocity started at 1.00 km/h and was increased gradually by 0.1 km/h up to 1.4 km/h.
The active-assist and passive mode were systematically provided from 100% (passive mode) to 0% (active-assist mode) assistance, as the system compensated the weight, resistance, and inertia in an optimal gait pattern.
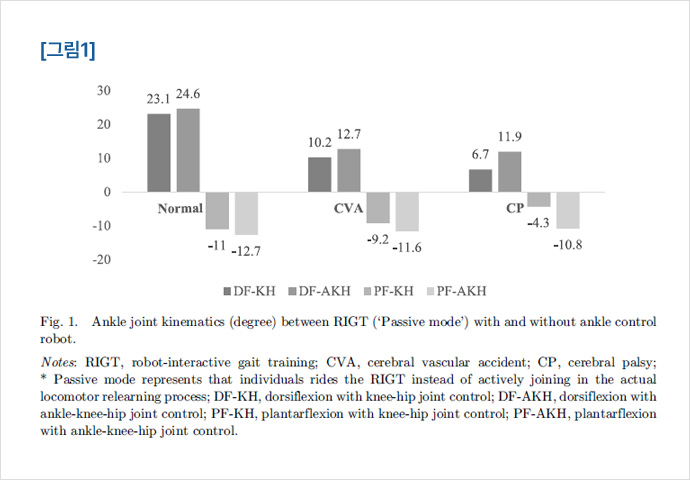
In healthy subjects, dorsiflexion and plantarflexion joint angles of the dominant leg were increased to a greater extent, by 6% and 13.4%, respectively, during RIGT with ankle control actuator than those during RIGT without ankle control actuator during the passive mode.
In patients with left hemiparetic stroke during the passive mode RIGT with ankle control actuator, the improvement of the affected side was 19.6% and 20.7% greater for ankle dorsiflexion and plantarflexion, respectively, than RIGT without ankle control actuator. During the passive mode in RIGT with ankle control actuator in patients with spastic diplegic CP, RIGT the improvement of the affected side was 43.6% and 60.1% greater for ankle dorsiflexion and plantarflexion, respectively, than those during RIGT without ankle control actuator (Fig. 1).
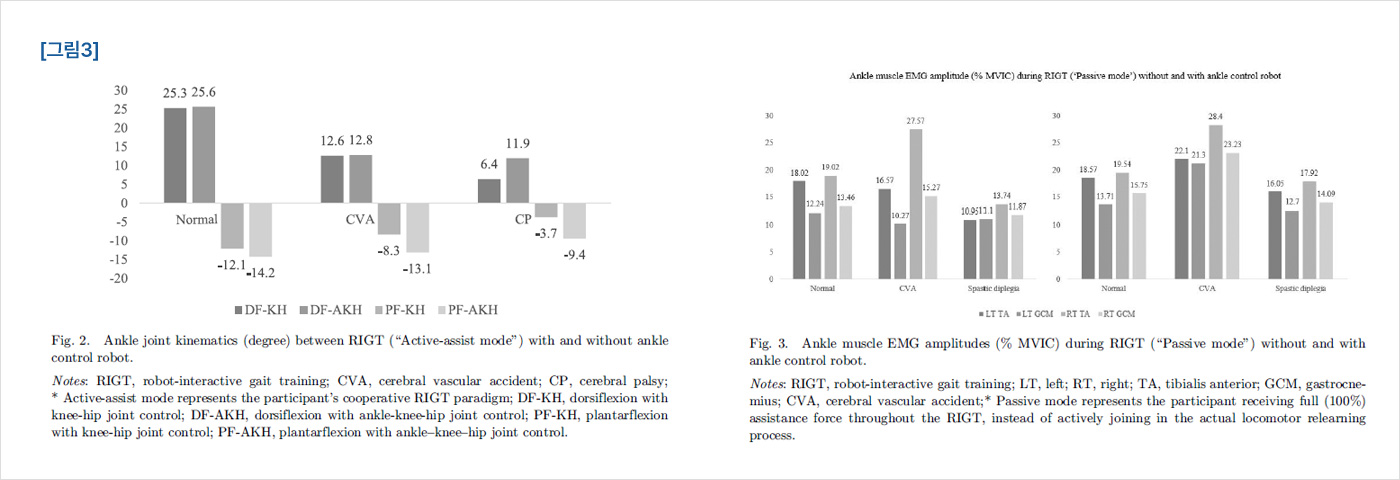
In healthy subjects, dorsiflexion and plantarflexion joint angles of the dominant leg were increased by 1.2% and 8.2%, respectively, during RIGT active-assist mode with ankle control actuator than RIGT without ankle control actuator.
In hemiparetic stroke cases, ankle dorsiflexion and plantarflexion increased by 1.5% and 36.6%, respectively, during active-assist mode RIGT with ankle control actuator, than RIGT without ankle control actuator.
In patients with spastic diplegic CP, during the active-assist mode, RIGT with ankle control actuator, ankle dorsiflexion, and plantarflexion was increased by 46.2% and 65.7%, respectively, than RIGT without ankle control actuator (Fig. 2).
In healthy subjects, during passive mode RIGT with ankle control actuator, TA and GCM muscle activity on the dominant leg was increased by 3% and 12%, respectively, RIGT than those during RIGT without ankle control actuator.
In stroke hemiparetic patients, during passive mode RIGT with ankle control actuator, TA and GCM muscle activity on the affected leg was increased by 25% and 51%, respectively, than that of RIGT without ankle control actuator.
In patients with spastic diplegia, TA and GCM muscle activity of the leg with the more significant deficit was increased by 31.8% and 12.6%, respectively, during passive mode RIGT with ankle control actuator than that of RIGT without ankle control actuator (Fig. 3).
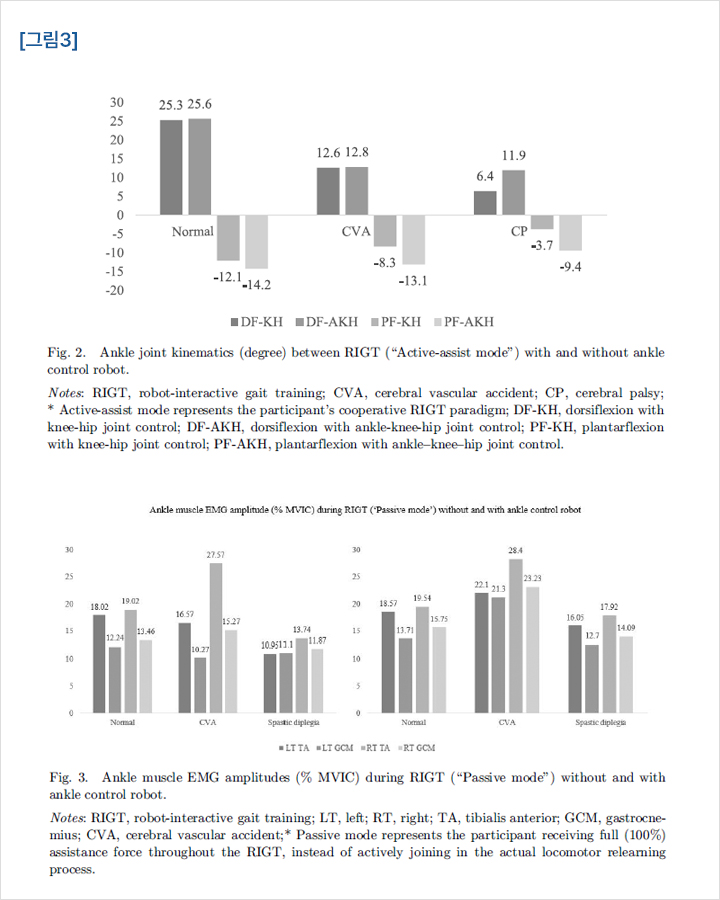
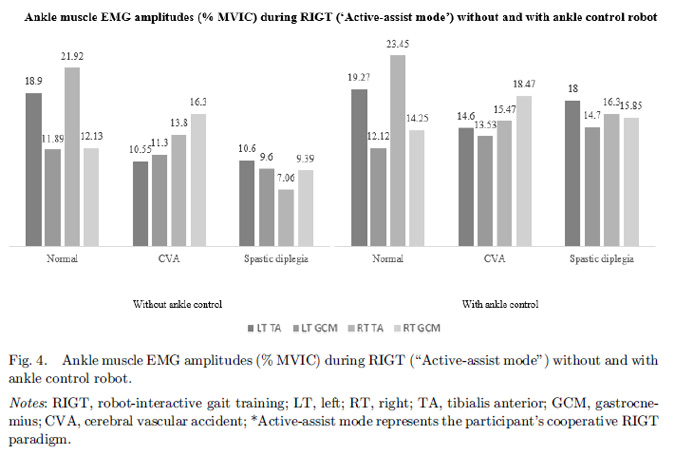
In healthy subjects, during passive mode RIGT with ankle control actuator, TA and GCM muscle activity of the dominant leg was increased each by 1.9% RIGT than that of RIGT without ankle control actuator.
In patients with hemiparetic stroke, during passive mode RIGT with ankle control actuator, activities of the TA and GCM muscles of the leg with greater deficits were increased by 27.7% and 16.4%, respectively, than those of RIGT without ankle control actuator.
In patients with spastic diplegia, during passive mode RIGT with ankle control actuator, activities of the TA and GCM muscles of the leg with greater deficits were increased by 41.1% and 34.6%, respectively, RIGT than those of RIGT without ankle control actuator.
As hypothesized, all the groups (healthy adults and participants with hemiparetic stroke or CP) with actuator presented superior results of TA and GCM muscle activities and joint kinematics both in the passive and active modes participant.
In the present study, RIGT the ankle muscle EMG data analysis demonstrated during RIGT with ankle joint actuator control, improved the TA and GCM muscle activities by 28.4% and 31.8%, respectively, than those during RIGT without ankle joint actuator control. The current finding suggests that RIGT with ankle control actuator is a valuable therapeutic tool for improving the isolated ankle dorsiflexion and plantarflexion movements necessary for locomotion in participants with brain damage. Furthermore, RIGT with ankle joint actuator control provides accurate, coordinated hip, knee, and ankle inter-joint muscle control; thus, it can be applied in preventing ankle plantarflexed gait (i.e., foot-drop gait), flexed-knee gait, and flexed/internal rotated-hip gait.
Our result was consistent with a previous ankle EMG study that compared the application of robotic ankle exoskeleton and unpowered ankle exoskeleton in women and reported an increase of 67% and 34% in ankle dorsiflexion and plantarflexion EMG activities, respectively, from heel contact to heel contact.
The EMG RMS amplitude was significantly increased by 18% in underactive TA and GCM, while decreased by 20%–30% in the overactive or hyperactive vastus lateralis and biceps femoris muscles.
This finding is an indication that ankle RIGT can also help to restore altered synergistic activation of the ankle and knee joint muscles.
As manifested in the brain damage cases, damage to the motor cortices and their descending corticospinal tracts results in muscle weakness, while brainstem descending pathways and the intraspinal motor network are disinhibited, leading to spasticity. Such neuromuscular impairments affect the ankle–foot interaction and the pelvic girdle movements (pelvic tilt, hip flexion, and adduction), and contribute considerably to the displacement of the center of gravity during walking.
The present result indicates that RIGT with ankle robotic control can provide accurate kinetic guidance force, which may facilitate appropriate proprioceptive feedback (e.g., ankle dorsiflexion and plantarflexion joint position, angle changes) during gait training.The post-intervention survey reported that the majority of participating participants experienced increased ankle position and movement sensory awareness from the enriched proprioceptive feedback on the ankle dorsiflexion and plantarflexion joint position, and kinesthetic sense. Such increased kinesthetic (movement) sensory awareness may have helped the participating participants to isolate better the ankle dorsiflexion and plantarflexion movement during RIGT with ankle joint actuator control than those during RIGT without ankle joint actuator control.
The clinical case series study demonstrated that RIGT with ankle control actuator is more effective in improving ankle EMG-controlled dorsiflexion and plantarflexion than RIGT without ankle control actuator in participants with stroke or CP.
Our results provided clinical evidence-based insights on the utilization of robot interactive locomotor training with ankle control to maximize and develop recovery of ankle–knee–hip joint movement control, thereby improving walking safety, preventing falls, and thus, improving the quality of life and the activities of daily living.