Clinical Research
Thank you for visiting the website of P&S Mechanics Co., Ltd.
Thank you for visiting the website of P&S Mechanics Co., Ltd.
We aimed to compare the effects of robotic assisted gait training (RAGT) in patients with FAC < 2 (low initial functional ambulation category [LFAC]) and FAC ≥ 2 (high initial functional ambulation category [HFAC]) on sensorimotor and spasticity, balance and trunk stability, the number of steps and walking distance in subacute hemiparetic stroke.
Fifty-seven patients with subacute hemiparetic stroke (mean age, 63.86 ± 12.72 years; 23 women) were assigned to two groups.
All patients received a 30-min Walkbot-assisted gait training session, 3 times/week, for 6 weeks.
Exoskeletal robotic-assisted gait training (RAGT) has rapidly gained popularity as a powerful and promising therapeutic modality to improve gait function in hemiparetic stroke; however, the best time to intervene and initial locomotor motor function level of patients for RAGT is unknown. A report from the National Rehabilitation Center recently emphasized the need to assess the characteristics leading to the best effectiveness and optimal timing, intensity, and duration of post-stroke RAGT rehabilitation interventions. Determining the patient’s initial ambulation level at which robot gait training is most effective remains problematic. Therefore, there is a need to determine the best functional ambulatory category (FAC) for more effective and sustainable RAGT intervention outcomes in stroke patients.
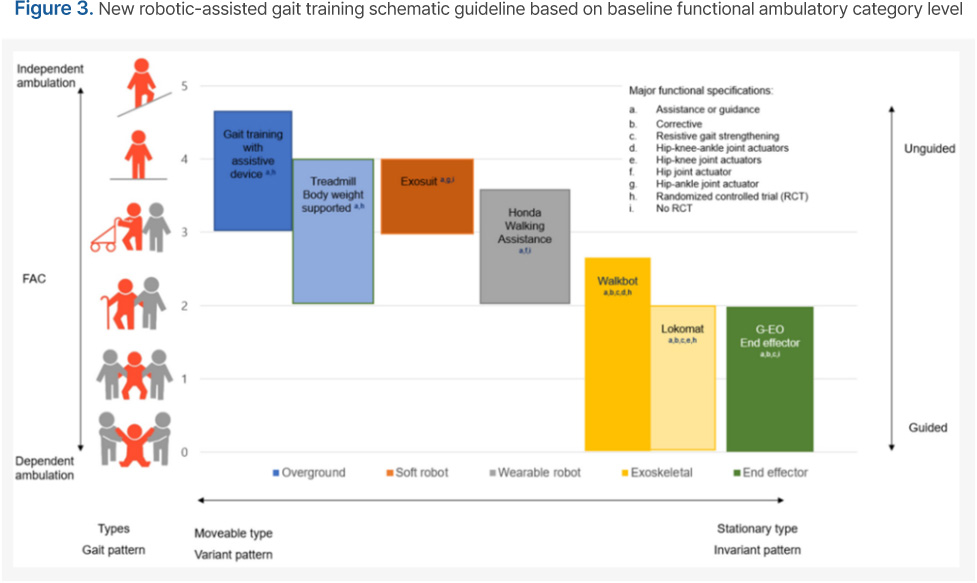
Morone proposed a conceptual scheme to classify the best robotic gait intervention types based on initial FAC in stroke robotic rehabilitation. Exoskeletal RAGT types, including the Lokomat (Hocoma, Zurich, Switzerland) and Walkbot (P&S Mechanics, Seoul, Korea), were suggested to be more effective in stroke patients with FAC < 2 (weight supporting group), whereas overground walking training was recommended for patients with FAC ≥ 2 (non-weight supporting group). An extensive systematic review of exoskeletal RAGT demonstrated that Lokomat and Walkbot have been commonly used to facilitate early mobilization using guidance mode (i.e., assist-as-needed) or impedance mode for stroke patients with FAC ≤ 2, showing varying results. Specifically, a study on the Lokomat RAGT in subacute stroke patients showed positive improvements in gait function. Walkbot RAGT studies consistently revealed positive improvements in balance and gait function in stroke patients. Recent clinical studies compared functional balance and lower extremity function outcome measures between Locomat and Walkbot robotic gait training in individuals with non-ambulatory chronic acquired brain injury patients, demonstrating equivalent results.
Specifically, we believe that the Walkbot interactive guidance mode can assist in mobilizing the ankle-knee-hip joint to facilitate the reciprocal interlimb-coordinated locomotor pattern for stroke patients with FAC < 2, while progressive resistance force (isokinetic) mode strengthens weak ankle-knee-hip muscles for stroke patients with FAC ≥ 2.
As these claims remain to be validated, the purpose of the present study was to determine the effects of Walkbot RAGT on sensorimotor recovery using the following outcomes:
Fugl–Meyer Assessment (FMA) scale scores, spasticity based on the Modified Ashworth Scale (MAS), balance based on the Berg Balance Scale (BBS), and trunk stability based on the Trunk Impairment Scale (TIS), as well as the number of steps and walking distance in subacute stroke patients with FAC < 2 (low initial functional ambulation category [LFAC]) and FAC ≥ 2 (high initial functional ambulation category [HFAC]).
We hypothesized that RAGT would produce equivalent improvements in sensorimotor recovery function based on FMA scale scores, spasticity based on MAS scores, alance based on BBS scores, and trunk stability based on TIS scores, as well as increased number of walking steps and walking distance in both groups.
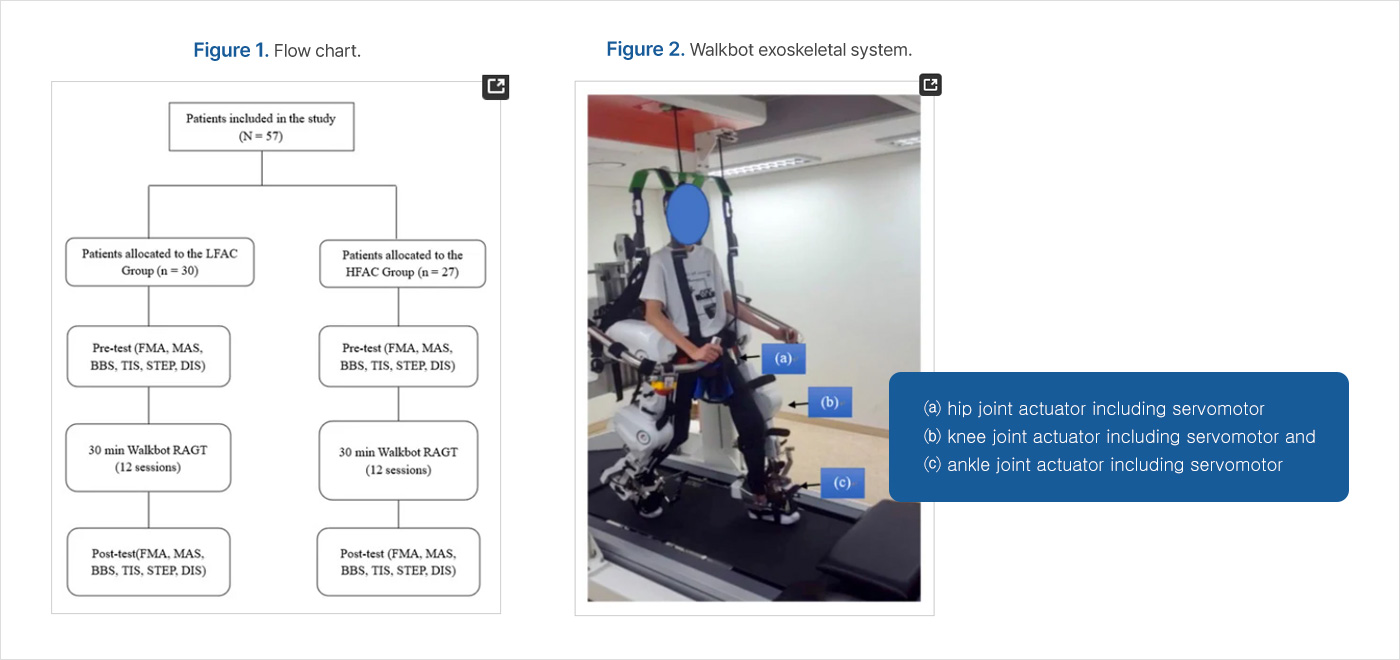
In this retrospective study, we included patients who took part in the RAGT intervention as inpatients in the Department of Rehabilitation Medicine at Cheong Dam Hospital in Seoul, Korea between June 2017 and September 2019. Fifty-seven patients with subacute stroke (mean age, 63.86 ± 12.72 years; 23 women) were assigned to two groups. The experimental study protocol was approved by the Cheong Dam Hospital Institutional Review Board and Ethics Committee (IRB No. CDIRB-2021-005). Informed consent was obtained from all patients prior to participation.
We included patients with subacute stroke who had been classified as FAC 0– 4 (FAC 0–1, [n = 30]; FAC 2–4, [n = 27]).
Both groups received the intervention three times/week every other day for six weeks (total: 18 sessions; minimum: 15 sessions) with a duration of 30 min (excluding set-up time) per session on the Walkbot-G system. Break time was provided whenever requested by the patient; however, the consecutive treatment time was maintained for at least 30 min. The Walkbot system is a robotic-assisted locomotor training device with built-in hip-knee-ankle inter-coordinated actuators to provide an optimal hip-knee-ankle-motion trajectory during locomotor training. An adjustable leg length and control of ankle-joint range of motion enables the Walkbot system to accurately approximate human kinematics and kinetics. This robotics system is designed to detect the patient’s gait characteristics in real-time (amount of participation or use in terms of active joint angular displacement excursion, active force/torque, and active weight-bearing center of pressure) and provides accurate and motivating real-time feedback concerning ankle-knee-hip kinematics and kinetics. Specifically, Walkbot RAGT can provide accurate proprioceptive, kinematic, and kinetic guidance, as well as variable error practice and high-intensity, repetitive, task-specific, and interactive exercises of the paretic lower limb. Initially, the RAGT body weight support (BWS) was set at 100%, which was gradually decreased until the knees started to collapse into flexion during the stance phase. The physical therapist monitored the knee condition and controlled the BWS throughout the sessions. Walking speed was initially set at 0.5 km/h and gradually increased until the patients self-selected a comfortable speed. The guidance force was maintained at 100% during training.
In addition to the Walkbot RAGT, both HFAC and LFAC groups consistently received conventional physical therapy (CPT), twice a day, 30 min per session. CPT was based on neurodevelopmental treatment (NDT) which includes mobility and stability exercises, ROM exercise, stretching and strengthening to futher enhance neurodevelopment. The investigators who performed all the evaluations were blinded to the interventions administered to both groups to minimize the experimenter bias where the physical therapists who provided the interventions did not involve in the assessments.
All patients who successfully completed the pre-test, intervention (at least 15 of 18 sessions), and post-test were included in the analysis. There were no significant differences in baseline age, height, weight, type of stroke, and side of hemiplegia distribution variables between the LFAC and HFAC groups. Baseline MAS, gait steps, and distance data were not significantly different, suggesting homogeneity of the groups. Baseline FMA, BBS, and TIS parameters were statistically different between groups. No safety issues were reported, and no patients experienced any side effects associated with RAGT.
ANCOVA test indicates the FMA score is significantly different between the LFAC group and HFAC group (p = 0.000) . Post hoc analysis confirmed that the intervention-related sensorimotor recovery was greater in the HFAC than LFAC (p = 0.000). However, the main effect of time was not a significantly different.
ANCOVA analysis indicates that the MAS are not significantly different between LFAC group and HFAC group, and time/Walkbot RAGT does not affect the MAS (p = 0.816) .
ANCOVA demonstrated that RAGT intervention significantly changed the main effect of time of BBS/balance in both the LFAC and HFAC groups (p = 0.000). The BBS scores/balance levels were significantly different between the LFAC and HFAC groups (p = 0.000). Post hoc analysis confirmed that the balance was greater in the HFAC than LFAC (p = 0.000).
ANCOVA results indicated that the RAGT intervention/time effect significantly changed the trunk stability/TIS scores in both the LFAC and HFAC groups (p = 0.026) and between the LFAC and HFAC groups (p = 0.000).
In addition, Post hoc analysis confirmed that the trunk balance was greater in the HFAC than LFAC (p = 0.001).
ANCOVA demonstrated significant main effects of time in both the LFAC and HFAC groups (p = 0.000), but no group main effect was observed (p = 0.482). In addition, post hoc analysis confirmed a main effect of time, but there were no significant differences between groups.
ANCOVA showed a significant main effect of time in both the LFAC and HFAC groups (p = 0.000), but no group main effects were observed (p = 0.593). Furthermore, post hoc analysis confirmed a main effect of time, but there were no significant differences between groups.
As anticipated, regardless of the baseline FAC, both groups demonstrated significant improvements in sensorimotor, spatiotemporal, loss of balance, and trunk stability function following Walkbot RAGT intervention. Most importantly, the current findings dispute the notion that exoskeletal RAGT using Walkbot can provide clinically meaningful changes in balance and gait function in subacute hemiparetic stroke patients with low or high initial FAC.
The functional score improvement amount analysis of the FMA sensorimotor function demonstrated an improvement in the functional score in the HFAC group (3.78) compared to that in the LFAC group (2.77), suggesting that RAGT was more beneficial for those with high initial ambulation ability than for those with low initial ambulation ability. Kim and colleagues (2020) reported that RAGT-induced sensorimotor recovery in FMA was approximately 13.04% greater than that of conventional physical therapy in 30 subacute stroke patients. A similar improvement in FMA (18.27%) was observed after 4-week RAGT compared to that of conventional physical therapy in 34 subacute hemiparetic patients. Such sensorimotor recovery may be associated with contemporary neurophysiological evidence of locomotor task-related neuroplasticity. Recent neurophysiological motor evoked potential evidence confirmed a positive correlation between FMA score and corticospinal excitability in the affected side of the primary motor cortex (M1) after RAGT in 13 patients with hemiparetic stroke.
Similarly, functional near-infrared spectroscopy neuroimaging data revealed 10–20% meaningful improvement in sensorimotor cortex (SMC), premotor cortex, and supplementary motor area network activation during RAGT in 15 subacute hemiparetic patients.
Static, dynamic balance, and trunk stability analyses showed significant time and group effects, indicating that those with high initial FAC showed greater improvement in the functional static and dynamic balance (11.71) and trunk stability (3.85) scores than those with low initial FAC dynamic balance (4.03) and trunk stability (0.90).
A remarkable enhancement in BBS score was shown with an increase from 6.6 to 26 after RAGT compared to that of conventional physical therapy in 14 subacute hemiparetic patients. Concurrently, trunk stability analysis revealed a moderate improvement (6.57%), which is compatible with previous TIS enhancement with RAGT (12.75%). A possible rationale for such improvement may be that Walkbot RAGT allowed patients to regain trunk stability because they were required to maintain upright postural stability while actively reciprocating the upper and lower limbs during locomotor training.
Spatiotemporal gait analysis showed a significant main effect of time in number of walking steps and walking distance in both the LFAC and HFAC groups (both p = 0.000). Such spatiotemporal gait improvement may have resulted from the fact that Walkbot RAGT provided an ample number of accurate, repetitive practice with a progressive passive-guided interactive isokinetic practice mode based on the individual’s initial FAC and sensorimotor conditions. Diserens and colleagues suggested that the accurate, repeated practice of locomotor behavior using RAGT may have facilitated the long-term potentiation underpinning synaptic neural plasticity, unmasking of the underutilized neural circuits, or utilization of the alternative neuronal pathways (e.g., ipsilateral corticospinal tracts, supplementary motor areas, and premotor cortex areas), which enhanced sustainable functional gait function recovery as evidenced by measurement of spatiotemporal gait.
This clinical research study demonstrated functional score improved sensorimotor, balance, trunk stability, number of steps, and walking distance in LFAC and HFAC patients recovering from subacute stroke. The present results provide clinical evidence-based insights into the utilization of RAGT in patients with different initial FACs to maximize functional score improvement of sensorimotor and trunk stability, as well as balance, the number of steps, and walking distance functions in neurorehabilitation in subacute stroke survivors.